


: “The Olodo Uprising: Pedagogical Challenges of Climate Change Education in an Era of Misinformation”
Option 2 (Direct and professional): “The Olodo Uprising: Addressing Climate Change Education Amidst Widespread Misinformation”
Option 3 (Concise): “The Olodo Uprising: Teaching Climate Science in an Age of Disinformation”
Recommendation: Option 1 is the standard tone for academic journals or formal reports.")



The Complexity of Health Misinformation: Why Susceptibility is More Than Just “Belief”
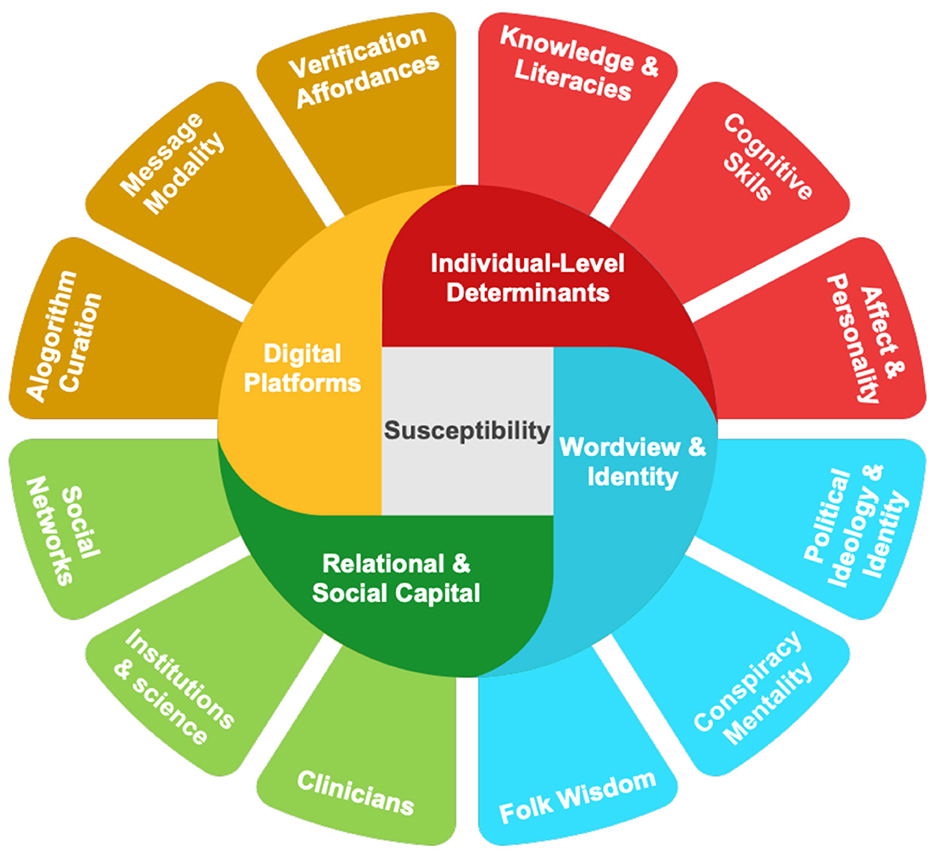
Health misinformation—information that contradicts scientific consensus—has become a defining public health crisis. While traditionally dismissed as a consequence of low intelligence or poor education, modern research reveals that susceptibility is a multifaceted phenomenon. It is not a binary state of “believer versus non-believer,” but a dynamic process shaped by how individuals navigate complex, high-stakes information environments. Current evidence suggests that susceptibility is best understood across three analytical levels: dispositional traits (like literacy and cognitive style), situational states (such as emotional salience and message framing), and the process of engagement (selection, evaluation, and reaction). This framework explains why even individuals with high cognitive abilities can fall prey to misinformation, particularly when their analytical skills are deployed to defend identity-based beliefs.
Measurement of this vulnerability has evolved from simple “fact-checking” quizzes to nuanced, multidimensional assessments. While early studies relied on static surveys to rate the accuracy of specific myths, experts now utilize Signal Detection Theory to disentangle “discrimination ability”—the genuine capacity to tell truth from fiction—from “response bias,” which is the tendency to accept information based on ideological alignment or group identity. Recent research further differentiates between distinct user profiles, ranging from “immune” individuals to “amplifying” publics who actively propagate false claims. By employing latent profile analysis, researchers can now identify which subsets of the population are most vulnerable, recognizing that those who feel they are “expert” or highly literate often suffer from an overconfidence gap, making them less likely to engage in necessary fact-checking.
A critical finding in the literature is that traditional “remedies,” such as increasing health or digital literacy, are insufficient on their own. While foundational knowledge is protective, it acts as a “resource” rather than a “silver bullet.” In some cases, high media literacy can even prove to be a double-edged sword; individuals with high evaluation skills may be better at identifying misinformation, yet they are also more prone to the “continued influence effect,” where they struggle to discard false information once it has been integrated into their worldview. Furthermore, self-perceived literacy often correlates with the Dunning-Kruger effect, where overconfident users are less vigilant than those who recognize their own limitations, leaving them particularly vulnerable to sophisticated AI-generated content.
Relationships and social trust often outweigh factual knowledge as predictors of susceptibility. Trust acts as a form of “social-epistemic capital,” determining whether an individual accepts an expert consensus or rejects it in favor of alternative narratives. Interpersonal trust in clinicians is one of the strongest protective factors against misinformation, as it is grounded in personal, consistent care. In contrast, institutional trust—such as confidence in government or public health agencies—is highly sensitive to political polarization. When individuals feel alienated from these authorities, they often turn to identity-aligned networks where false information is not only circulated but legitimized by trusted peers. In these community-based networks, sharing misinformation is frequently an act of social bonding or altruism rather than a deliberate attempt to deceive.
Digital platforms and environmental factors serve as “susceptibility multipliers” that radically reshape how health information is processed. Algorithmic environments and “news-finds-me” perceptions—the belief that one does not need to actively seek news because it will appear on their feed—encourage passive, heuristic consumption. When this is paired with emotionally vivid content like deepfakes or anxiety-inducing videos, it forces the brain into a state of high arousal and narrow focus, which suppresses the desire to verify facts. The interaction between human psychology and platform design is critical; even a highly motivated user may succumb to misinformation if the platform utilizes verification cues (like checkmarks) that effectively bypass critical thinking or exploit a user’s perceived sense of digital self-efficacy.
Ultimately, addressing the epidemic of health misinformation requires shifting from one-size-fits-all fact-correction toward tailored, structural interventions. Solutions must move beyond “debunking” toward strategies that acknowledge the configurational nature of belief. For clinicians, this means prioritizing the preservation of patient-provider trust as a foundational barrier against misinformation. For policymakers and platform designers, it requires a focus on systemic changes that slow the velocity of information sharing, label uncertainty, and reduce information overload. By understanding that susceptibility is a product of social identity, emotional needs, and platform architecture, stakeholders can design interventions that address the reasons why people believe misinformation, rather than simply labeling them as misinformed or uneducated.

: “The Olodo Uprising: Pedagogical Challenges of Climate Change Education in an Era of Misinformation”
Option 2 (Direct and professional): “The Olodo Uprising: Addressing Climate Change Education Amidst Widespread Misinformation”
Option 3 (Concise): “The Olodo Uprising: Teaching Climate Science in an Age of Disinformation”
Recommendation: Option 1 is the standard tone for academic journals or formal reports.")

